TOGETHER WE CAN
Community Based Sustainable Tele-Chronic Disease Management
A Project of Bangladesh Medical Association on North America-Louisiana Chapter (BMANA-LA).
Community Based Sustainable Tele-Chronic Disease Management: A Pilot Project Proposal on Hypertension
In a remote community in Rajshahi, Bangladesh, a small business owner named Kalam, in his late fifties has been suffering from long-standing diabetes. He has been taking health service from local diabetes center, but he received minimal blood tests, few medications, and inconsistent follow up service. His health has not improved and gradually his vision became blurry, feet started hurting, and was feeling tired more often. He is the main bread earner of his family and was worried of what would happen to his family if he is not him. Therefore, he resorted to a relative, who is also local medical personnel, who gave him a revised prescription. He perceives that he is better than the doctors at the diabetes center. When asked to take regular blood glucose measurement, he said he will go to his next-door neighbor. His neighbor has blood glucose measurement machine and helps him in the process. However, nothing is in place to ensure routine check-up. He only checks when he is not feeling well. He Kalam’s long standing diabetes, if not well controlled, puts him in increased risk of heart attack, stroke, and kidney disease, which he does not know.
Kalam’s story is a glimpse of many people struggling with chronic diseases, such as hypertension, high cholesterol, and diabetes, in developing countries. Bangladesh is one of those countries, with limited health care access to people, particularly those living rural and remote areas. While many may think that infectious diseases comprise main health burden in Bangladesh, chronic diseases and complications of chronic diseases account for half of the morbidity and mortality in the country (please see below for further statistical data). Furthermore, due to lack proper awareness and monitoring service, many people, particularly the marginalized ones, experience stroke, heart attack, and kidney failure and face untimely death. Families struggle when loved ones die or incur paralysis from these complications, often without knowing the contributing cause.
Kalam’s story also illustrates the power of social networks to meet health care needs. Kalam resorts to his medical personnel relative to revise prescription of a doctor, and his next-door neighbor to help him monitor blood glucose. Together they support him to help him overcome his barriers to health, and support to keep him healthy. This natural practice has led us to consider following possibilities:
What if a health care service taps into the power of collective action among residents in a community?
What if a health care service strongly considers residents barriers and promotes collective capacity to overcome them?
What if a service actively searches of trusted altruistic leaders as opposed to political interest driven leaders to help coordinate care?
What if the service employs a technology integrated with the local context to continuously monitor chronic disease states and intervenes before it is too late?
Our model of chronic disease management builds from understanding a community. With that understanding, it involves patients’ close social networks to help meet treatment goals, and technology to enable providers remotely monitor chronic disease status. First, we aim to conduct ethnographic description of a community to understand the community. Then, we identify close social networks of patients with known chronic disease status to facilitate collaborative actions among them to support the patients. Lastly, we involve trusted leaders endorsed by the patients to coordinate weekly insertion of chronic disease measurement data, such as blood pressure or blood glucose measurement, in a secured computer remotely accessible to providers. The measurement data is to be monitored by the providers. The providers work with the collaborative network to help meet patients’ goals.
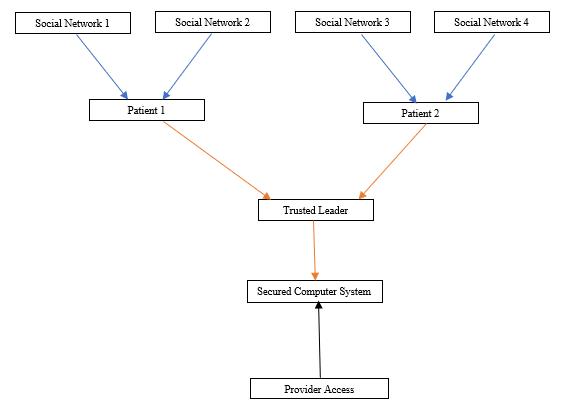
=Collaboration among patient and social networks
= Blood pressure measurement data flow
= Provider’s remote access.
Figure: A Diagrammatic Representation of Our Model.
Our model recognizes that many aspects of chronic disease management, such as buying medicine, remembering to take medicine, and lifestyle changes, are primarily driven by patients. Promoting collective capacity by involving patient’s close social network can be a powerful tool help people take ownership of their own care. Furthermore, technology can be used to remotely monitor patients’ chronic disease status regularly to provide early intervention whenever necessary.
Establishing continuous health care access across communities is our ultimate mission. We want to start in a community at a small scale to establish a model. Then, we want to replicate and expand to systematically engage with other communities to improve chronic disease status across Bangladesh and beyond. By delivering timely intervention to chronic disease problems, we believe that we will be able to help many families who may lose their loved ones early from stroke, heart attacks, and kidney failure.
Our pilot project will be implemented at Khorigapara community located at Godagari subdistrict in Rajshahi, Bangladesh addressing hypertension. Health care access is considered as one of the pressing felt need by residents living there. Please consider more data about the community, current evidence of our model, and description of our project below. You can also download our complete project here.
The needs for sustainable and continuous health care access for chronic diseases are enormous among marginalized communities. Your little help can make a establish lasting access of health care across communities.
We truly count on your generous donation!